
Ashtamgam Ayurveda Chikitsalayam
India/Kerala/Palakkad
Starting Rate Per Night: ₹ 3,000

Ashtamgam Ayurveda Chikitsalayam & Vidyapeedham is a distinguished centre for authentic Ayurvedic healing and classical education, located in the serene foothills of Nagalassery, Kerala. Established in 2011 under the...

When Central Vision Blurs: An Ayurvedic Path to Eye Health Support and Visual Preservation
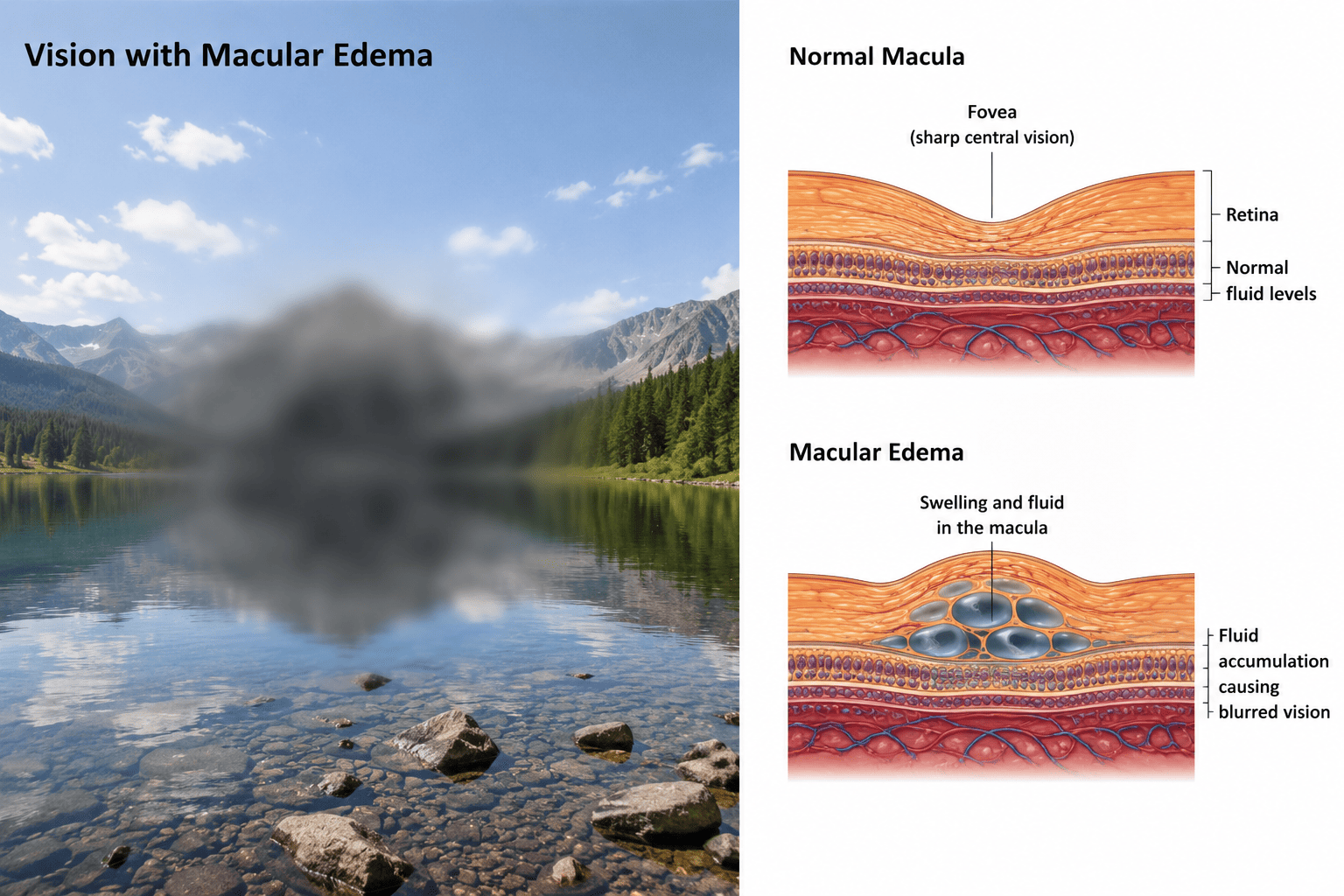
The macula — that small central area of the retina just a few millimetres across, densely packed with millions of cone photoreceptors — is responsible for the sharpest, most detail-rich vision the human eye possesses. The faces we recognise, the words we read, the colours we perceive, the fine work of every day, the central focus that holds our visual world together — all depend on this remarkable concentration of specialised neural tissue. When fluid accumulates within or beneath the macula — disrupting the precise layered architecture of this delicate area, separating photoreceptors from the underlying retinal pigment epithelium, distorting the geometry on which sharp vision depends — central vision blurs, distorts, and fades in ways that surface treatment alone cannot easily restore. Macular Edema is the swelling of the macula from abnormal fluid accumulation, and it represents one of the leading causes of vision impairment in working-age adults globally, particularly in diabetic retinopathy where it affects a substantial proportion of patients and is the principal cause of vision loss in diabetic eye disease.
The causes are varied, and the pathophysiology depends substantially on cause. Diabetic Macular Edema (DME) — the most common form globally — develops when chronic hyperglycaemia damages retinal blood vessels, with breakdown of the blood-retina barrier, increased vascular permeability, and leakage of fluid, lipids, and proteins into the macular tissue. The damage involves both microvascular pathology (capillary closure, microaneurysms, hard exudates) and a substantial inflammatory component now well-recognised. DME is one of the leading causes of preventable blindness in working-age adults globally, making it one of the most clinically important retinal conditions to manage well. Retinal Vein Occlusion (RVO) — both central retinal vein occlusion (CRVO) and branch retinal vein occlusion (BRVO) — produces macular edema through impaired venous drainage with increased hydrostatic pressure forcing fluid into retinal tissue. Uveitic Macular Edema complicates chronic uveitis through the broader inflammatory process disturbing the blood-retina barrier and macular fluid balance. Post-Surgical Cystoid Macular Edema (Irvine-Gass syndrome) develops in some patients after cataract surgery, typically 4 to 12 weeks postoperatively, through inflammatory mediators released during and after surgery. Wet Age-Related Macular Degeneration involves choroidal neovascularisation (abnormal new vessel growth from the choroid through Bruch's membrane into the subretinal space) with consequent leakage producing macular edema. Macular edema from other causes includes radiation retinopathy following ocular or head-and-neck radiotherapy, hypertensive retinopathy in severe uncontrolled hypertension, drug toxicity (certain chemotherapy agents, taxanes, niacin in high doses, glitazones, fingolimod, and others), epiretinal membrane traction, vitreomacular traction syndrome, retinitis pigmentosa-associated macular edema, and various rarer aetiologies.
Modern ophthalmology has transformed macular edema treatment over the past two decades — perhaps no area of eye disease has seen as dramatic an improvement in outcomes as macular edema management since the introduction of anti-VEGF therapy. Anti-VEGF therapy — intravitreal injections of ranibizumab, aflibercept, bevacizumab (off-label but widely used), brolucizumab, and faricimab — has become the cornerstone of treatment for diabetic macular edema, RVO-related edema, and wet AMD-related edema. These agents block vascular endothelial growth factor (VEGF), the key driver of pathological vascular permeability and neovascularisation, often producing remarkable visual recovery in patients who decades ago would have progressed to legal blindness. Intravitreal steroid implants (dexamethasone sustained-release implant, fluocinolone acetonide implant) provide longer-duration anti-inflammatory therapy in selected cases. Focal/grid laser photocoagulation remains useful in selected DME presentations, particularly for non-centre-involving DME. Surgical intervention (vitrectomy with internal limiting membrane peel) is reserved for specific cases including macular edema with significant vitreomacular traction or epiretinal membrane component. Treatment of underlying systemic conditions — optimal diabetes management for DME, treatment of underlying inflammation for uveitic macular edema, blood pressure control for hypertensive contributions — is essential alongside the specific retinal interventions.
These approaches are absolutely cornerstone, often vision-saving, and must never be delayed or substituted by anything else. This bears emphasis: for active macular edema with vision impairment, anti-VEGF treatment (where indicated by the specific cause and clinical pattern) is genuinely transformative and Ayurveda has no role in replacing it. Delay of indicated anti-VEGF treatment can result in irreversible vision loss as the chronic edema produces permanent photoreceptor damage. The patient considering integrative care must understand this absolutely clearly from the outset.
Yet within this honest framing, a real therapeutic gap exists for many macular edema patients. The patient with diabetic macular edema requiring monthly anti-VEGF injections for years remains on the injections in part because the underlying systemic diabetic and inflammatory background that drives the macular pathology continues unabated. The injection schedules represent maintenance against an ongoing systemic process rather than resolution of it. The patient whose response to anti-VEGF is incomplete — with persistent residual macular thickness on OCT despite optimised injection schedules — has limited additional options. The patient with chronic recurrent macular edema seeks to address the systemic root rather than only the macular consequence. The broader question — how do I support the metabolic, vascular, and inflammatory background that perpetuates macular edema, alongside the essential anti-VEGF treatment that addresses the macular consequence — remains substantially unanswered by retinal-level intervention alone.
This is where Ayurveda offers a thoughtful, clinically grounded contribution within clear limits. Macular edema fundamentally requires ophthalmological treatment, and active macular edema with vision impairment requires anti-VEGF therapy where indicated — there is no Ayurvedic substitute for this. What Ayurvedic care offers, working alongside conventional treatment, is meaningful supportive value: addressing the systemic metabolic and vascular background that drives the macular pathology (particularly important in diabetic patients where the systemic Madhumeha dimension is the root); reducing the chronic systemic inflammatory burden contributing to retinal vascular dysfunction; supporting overall ocular tissue health through classical Triphala-Saptamrita Lauha-Amalaki antioxidant therapy that aligns conceptually with the antioxidant logic of modern AREDS2 supplementation; addressing Punarnava-specific fluid-clearing classical pharmacology relevant to the edema dimension; supporting Alochaka Pitta balance (Ayurveda's framework for the Pitta sub-form governing visual function); and providing the deeper constitutional rebuilding through Rasayana therapy that conventional ophthalmological treatment alone does not address. By understanding macular edema within the broader Drishti Vikara framework, addressing the Pitta-Kapha-Rakta-Vata combinations specific to each cause, and integrating systemic doshic care with eye-specific therapy, Ayurvedic treatment provides a meaningful complement to modern ophthalmology.
A Macular Edema treatment retreat is best understood as integrative supportive care for patients undergoing ongoing ophthalmological treatment, never as primary therapy or substitute for anti-VEGF injections — particularly valuable for diabetic macular edema patients where the systemic metabolic dimension is substantial, and for chronic recurrent macular edema patients seeking to address the deeper systemic background alongside continued retinal care.
What is Macular Edema?
Macular Edema is abnormal fluid accumulation within the layers of the macula or in the subretinal space beneath it — disrupting the precise architecture of the central retina responsible for sharp central vision. The fluid distorts the normal layered organisation of the macular tissue, separates photoreceptors from their critical relationship with the retinal pigment epithelium, and compromises the function of the most visually important region of the retina. Chronic untreated macular edema causes progressive photoreceptor damage that can become permanent, making timely treatment essential for preserving vision.
The fluid in macular edema can be located in different compartments of the macular tissue:
Intraretinal fluid — Within the layers of the retina itself, typically appearing as cystoid spaces on optical coherence tomography (OCT). This is the most common pattern in diabetic and RVO-related macular edema.
Subretinal fluid — Beneath the neurosensory retina, between the retina and the retinal pigment epithelium. Common in wet AMD-related macular edema and certain other presentations.
Sub-RPE fluid — Beneath the retinal pigment epithelium, often associated with pigment epithelial detachment in wet AMD.
Principal causes:
Diabetic Macular Edema (DME) — Most common cause globally and a leading cause of preventable vision loss in working-age adults. Develops in diabetic retinopathy from chronic hyperglycaemia-induced microvascular damage with breakdown of the blood-retina barrier. Can be classified as centre-involving DME (affecting the foveal centre) or non-centre-involving DME, with treatment approach differing based on this distinction. Closely linked to overall diabetes control (HbA1c), diabetes duration, blood pressure, lipid status, and other systemic factors.
Retinal Vein Occlusion (RVO) — Both central retinal vein occlusion (CRVO, affecting the main retinal vein draining the entire retina) and branch retinal vein occlusion (BRVO, affecting a tributary draining a quadrant of the retina) commonly cause macular edema through impaired venous drainage. Risk factors include hypertension, hyperlipidaemia, diabetes, glaucoma, hypercoagulable states, and atherosclerosis.
Uveitic Macular Edema — Common complication of chronic uveitis (intermediate, posterior, and panuveitis particularly), where the broader inflammatory process affecting the eye disturbs the blood-retina barrier and produces macular fluid accumulation. Particularly significant in conditions like Behçet's disease, sarcoidosis-related uveitis, and chronic idiopathic uveitis.
Post-Surgical Cystoid Macular Edema (Irvine-Gass Syndrome) — Develops in some patients after cataract surgery, typically 4 to 12 weeks postoperatively. Inflammatory in origin, often responsive to topical NSAID and steroid therapy, occasionally requiring intravitreal intervention.
Wet Age-Related Macular Degeneration — Choroidal neovascularisation (abnormal vessels growing from the choroid through Bruch's membrane) produces exudation into the macular tissue, with both intraretinal and subretinal fluid components possible. Anti-VEGF therapy is the cornerstone of wet AMD treatment.
Radiation Retinopathy — Following ocular or head-and-neck radiotherapy, with macular edema developing months to years after exposure.
Hypertensive Retinopathy — Severe uncontrolled hypertension can produce macular edema along with other hypertensive retinal changes.
Drug-Induced Macular Edema — Various medications can produce macular edema as an adverse effect, including certain chemotherapy agents (taxanes), niacin in high doses, thiazolidinediones (glitazones used in diabetes), fingolimod (used in multiple sclerosis), prostaglandin analogues used in glaucoma (occasionally), and others. Recognition and discontinuation of the offending agent is essential.
Epiretinal Membrane and Vitreomacular Traction-Associated Edema — Mechanical traction from epiretinal membrane or abnormal vitreomacular attachment can produce macular distortion and edema, often requiring surgical management.
Retinitis Pigmentosa-Associated Cystoid Macular Edema — Affects a subset of patients with retinitis pigmentosa.
Other Causes — Including post-occlusion macular edema after retinal artery occlusion (less common than RVO-related), inflammatory conditions (multifocal choroiditis, birdshot chorioretinopathy), genetic conditions (juvenile X-linked retinoschisis with macular component), and various rarer aetiologies.
Common symptoms include blurred or distorted central vision (often the first noticed symptom), metamorphopsia (straight lines appearing wavy — classically tested with the Amsler grid), faded or washed-out colours, central scotoma (a blind spot in the central visual field), difficulty reading and recognising faces, reduced contrast sensitivity, and in some patients micropsia (objects appearing smaller than they are). Symptoms typically develop over weeks to months in chronic macular edema, more rapidly in acute wet AMD or Irvine-Gass syndrome.
Diagnosis: Optical coherence tomography (OCT) is the gold-standard investigation for macular edema, providing detailed cross-sectional imaging of macular structure with quantification of macular thickness and visualisation of fluid location. OCT is essential for both initial diagnosis and ongoing monitoring of treatment response. Fluorescein angiography identifies sources of leakage and is particularly useful in DME and RVO. OCT angiography is increasingly used as a non-invasive alternative for assessing macular and choroidal vasculature. Amsler grid for patient self-monitoring at home. Systemic evaluation identifies underlying cause and contributing factors — diabetes assessment, blood pressure, lipid panel, inflammatory markers where indicated.
Understanding Drishti Vikara and Alochaka Pitta Dushti: The Ayurvedic Root of Macular Edema
In Ayurveda, retinal and macular disorders fall within the broader category of Drishti Vikara (visual function disorders) and the deeper classical category of Sarvagata Netra Roga (whole-eye diseases affecting the visual axis). The classical Ayurvedic understanding of vision and visual disorders is sophisticated, with detailed descriptions in Sushruta Samhita's Uttara Tantra and Madhava Nidana of various retinal-pattern conditions, fluid pathologies of the eye, and the doshic combinations that produce them. While classical Ayurveda did not have the modern technology to visualise the macula directly, the clinical descriptions of central vision impairment with various qualities, fluid-pathology presentations, and the doshic-systemic connections to eye disease provide a robust framework that maps meaningfully onto modern macular edema understanding.
The core pathophysiological concepts include:
Alochaka Pitta Disturbance — Alochaka Pitta is the sub-form of Pitta responsible for visual perception and the integrative function of vision. Disturbance of Alochaka Pitta produces the central vision impairment, blurring, distortion, and reduced colour saturation that characterise macular edema. The classical recognition that visual function depends on a specific Pitta sub-form aligns with the modern understanding that the macula has specific specialised physiological characteristics distinct from the rest of the retina, and that macular dysfunction has its own clinical signature.
Pitta-Rakta Vitiation in Inflammatory and Vascular Macular Edema — For inflammatory causes (uveitic macular edema, post-surgical Irvine-Gass), and for the inflammatory dimensions of diabetic macular edema (now well-recognised as having substantial inflammatory contribution), Pitta-Rakta vitiation drives the underlying pathology. The classical understanding of inflammatory eye conditions involves Pitta-Rakta combinations producing the heat, vascular dysfunction, and tissue damage that characterise these presentations.
Kapha-Driven Fluid Accumulation — The accumulation of fluid itself within macular tissue reflects Kapha excess at the local level. The classical understanding of fluid pathologies (Sotha) in various body regions, including the eye, provides framework for understanding pathological fluid accumulation in tissues that should be relatively fluid-free. The macular edema dimension specifically is the Kapha-fluid component of the broader doshic picture.
Vata Aggravation — Vata contributes to the progressive degenerative aspects, the unpredictable course, and the neurological-perceptual dimensions of chronic macular edema. In chronic recurrent cases requiring repeated anti-VEGF injections, the Vata aggravation that develops with chronic disease contributes to the constitutional depletion many patients experience.
Sannidana-Madhumeha Connection for Diabetic Macular Edema — For diabetic macular edema specifically, the classical Ayurvedic understanding recognises this clearly as a complication of Madhumeha (diabetes), with the systemic Kapha-Meda-Ama-Vata imbalance of long-standing diabetes producing Upadrava (complications) affecting the eye. This systemic-root framework provides a clear rationale for addressing the underlying Madhumeha alongside the eye-specific care — exactly the integrative approach that complements modern care which itself increasingly emphasises that optimal diabetes management is foundational to DME treatment.
Rakta Vaha Srotas Dushti — Vitiation of the blood circulation channels, central to all the vascular-driven macular edema presentations (DME with its microvascular damage, RVO with venous occlusion, hypertensive retinopathy, post-RVO chronic edema).
Ama and Mandagni in Systemic Background — Metabolic toxin accumulation and weak digestive fire contributing to systemic background, particularly relevant in DME where the broader metabolic dimension drives the retinal pathology.
Ojas Kshaya — Chronic systemic disease (long-standing diabetes, chronic uveitis, recurrent inflammation) depletes Ojas — the vital essence — including the ocular tissue Ojas that supports retinal cellular function and resilience.
Specific Predisposing Nidana — Classical texts identify factors that produce eye disorders: dietary indiscretions particularly Viruddha Ahara, excess sun exposure, exposure to heat, excessive visual strain, suppression of natural urges, emotional disturbance, and specific to modern relevance the recognition that chronic systemic illness produces eye complications through the Upadrava mechanism. For DME, the Madhumeha-driven systemic background and inadequate diabetes management are the principal modifiable Nidana.
The Punarnava-Fluid-Pathology Recognition — A particularly relevant classical pharmacological insight: Punarnava (Boerhavia diffusa) is the premier Ayurvedic herb for fluid-accumulation pathologies, with classical recognition of its specific action on Sotha (oedema and fluid pathology) including ocular fluid presentations. The integration of Punarnava-based therapy for macular edema represents one of the more direct classical-modern pharmacological alignments, with Punarnava's well-documented diuretic, anti-inflammatory, and tissue-protective actions providing meaningful supportive pharmacology for the edema dimension specifically.
This comprehensive understanding shapes the Ayurvedic approach to macular edema: address the systemic root particularly for diabetic and inflammatory presentations — managing Madhumeha optimally for DME, addressing inflammatory pathways for uveitic macular edema, managing vascular background for RVO-related edema; support overall ocular tissue through classical Triphala-Saptamrita Lauha-Amalaki Rasayana therapy that aligns with the antioxidant logic of AREDS2 supplementation; integrate Punarnava-based therapy specifically for the fluid-accumulation dimension; provide gentle classical eye-supportive therapy (Netra Tarpana with appropriate eye-protective ghees) when clinically appropriate and with ophthalmologist coordination; clear Ama and address Mandagni through systemic care; rebuild Ojas through sustained Rasayana — always alongside essential anti-VEGF and ophthalmological care, never as a substitute for it, and always with clear coordination with the treating ophthalmologist on injection scheduling and overall management.
The 3 Stages of Ayurvedic Treatment for Macular Edema
Ayurvedic care for Macular Edema follows a carefully sequenced three-stage approach, adapted at every step to the specific cause of macular edema, current anti-VEGF or other ophthalmological treatment schedule, OCT findings, underlying systemic conditions (particularly diabetes), and overall constitutional state. The approach is consistently integrative — undertaken alongside continued ophthalmological care, with all anti-VEGF injection schedules maintained without interruption.
1. Preparation (Purva Karma) The preparatory stage begins with thorough assessment including review of current OCT findings, anti-VEGF treatment schedule and response, diabetes control parameters (for DME patients), blood pressure status, other systemic factors, and constitutional profile. Deepana-Pachana (kindling the digestive fire and digesting Ama) addresses the metabolic background that contributes substantially to the inflammatory and vascular dimensions of macular edema, particularly important in DME. Internal Snehana (oleation) uses eye-supportive medicated ghees appropriate to the specific clinical pattern: Triphala Ghrita — the foundational eye-supportive ghrita with broad antioxidant and Rasayana action on ocular tissues; Mahatriphala Ghrita — a more concentrated eye-Rasayana preparation; Jeevantyadi Ghrita — particularly valuable for Pitta-dominant inflammatory presentations and for supporting the photoreceptor-RPE tissue layer; Patoladi Ghrita for combined Pitta-Kapha presentations. Dosing is calibrated to the patient's digestive capacity and metabolic state. Gentle external Abhyanga with appropriate medicated oils improves overall circulation and supports relaxation. For diabetic patients, the preparation stage includes optimisation of diabetes management in coordination with the diabetologist where this can be supported, recognising that improved glycaemic control is one of the most important modifiable factors for DME outcomes.
2. Core Treatment (Pradhana Karma) Primary therapies focus on three coordinated lines of action: systemic clearing through Virechana, classical eye-supportive therapy, and Punarnava-led specific pharmacology for the fluid dimension.
Virechana (therapeutic purgation) is the central systemic clearing therapy for macular edema, particularly valuable for the Pitta-Kapha-Ama background driving DME, the inflammatory dimensions of uveitic macular edema, and the broader metabolic burden in chronic recurrent presentations. Performed with classical herbal purgatives carefully selected for the patient's doshic profile (Trivrit Lehyam, Avipattikara Churna-based preparations, Triphala-based purgatives, or specific formulations matched to clinical state), Virechana clears systemic Pitta from the gut, liver, and circulation; reduces the inflammatory mediator burden contributing to retinal vascular dysfunction; addresses the metabolic-inflammatory background driving DME; and enhances the bioavailability and effectiveness of subsequently administered ocular-supportive herbal therapy. Dosing is calibrated carefully to the patient's overall state, with particular attention to diabetic patients where glycaemic state must be stable.
Classical eye-supportive therapy runs alongside:
Netra Tarpana — The classical Ayurvedic therapy involving retention of medicated ghee over the eye within a contained ring constructed on the face around the orbit — provides gentle, sustained therapeutic action on the ocular tissues including the cornea, conjunctiva, and through systemic absorption effects on broader ocular tissue health. For macular edema patients, Netra Tarpana is performed only when clinically appropriate and with ophthalmologist clearance, typically when the macular edema is stable (not in acute flare), at least 2 weeks after the most recent anti-VEGF injection, and with appropriate eye-protective ghee selection (Triphala Ghrita, Mahatriphala Ghrita, or Jeevantyadi Ghrita based on doshic pattern). The procedure is performed with proper aseptic technique by trained therapists. It is important to be clear: Netra Tarpana supports overall ocular tissue health and provides systemic ocular Rasayana effect but is not direct treatment for the macular edema fluid itself — that fluid is the target of anti-VEGF therapy. Netra Tarpana's role is supportive ocular care alongside the essential ophthalmological treatment.
Nasya — Marsha Nasya with Anu Taila supports the broader head-eye ecosystem and provides general Vata-pacifying and head-channel-clearing effect that supports overall eye health.
Systemic herbal therapy with the macular-edema-specific pharmacology forms the third cornerstone:
Punarnava (Boerhavia diffusa) — The premier Ayurvedic herb for fluid-accumulation pathologies, particularly valuable for the edema dimension of macular edema. Punarnava's classical action on Sotha (oedema) combined with its anti-inflammatory, tissue-protective, and mild diuretic properties provides supportive pharmacology specifically relevant to fluid-accumulation conditions including macular edema.
Triphala (Amalaki + Bibhitaki + Haritaki) — The foundational eye-supportive antioxidant combination with substantial modern research evidence for antioxidant action relevant to retinal oxidative damage. The high vitamin C content of Amalaki and the broader antioxidant action of the combination align conceptually with the antioxidant logic of AREDS2 supplementation in age-related retinal disease.
Saptamrita Lauha — The classical eye-protective combination integrating Triphala with Yashtimadhu and iron preparation, with traditional indications spanning multiple retinal and visual conditions.
Amalaki Rasayana — Provides sustained antioxidant and broader Rasayana support.
Guduchi (Tinospora cordifolia) — Immunomodulatory and anti-inflammatory action particularly relevant to inflammatory dimensions of macular edema and to the systemic inflammatory background in DME.
Haridra (turmeric) — Anti-inflammatory and antioxidant action with relevance to retinal inflammation.
Manjistha (Rubia cordifolia) — Rakta-shodhaka (blood-purifying) action with classical indication for inflammatory and vascular eye pathology.
Yashtimadhu — Broader Pitta-pacifying and anti-inflammatory action.
For diabetic patients, Madhumeha-specific herbs are integrated: Methi (fenugreek), Karela (bitter gourd), Vijaysar, Gudmar, and Jamun support glycaemic regulation alongside diabetes medications and complement the diabetic care.
Throughout the core treatment stage, anti-VEGF injection schedules continue uninterrupted. The Ayurvedic treatment timing is planned around the injection schedule, typically avoiding Netra Tarpana within 1-2 weeks of injection and avoiding any procedures that would interfere with the injection administration.
3. Rejuvenation (Paschat Karma) The final stage focuses on long-term supportive care and constitutional rebuilding through sustained Rasayana therapy with eye-protective and antioxidant medicines including continued Triphala, Saptamrita Lauha, Amalaki Rasayana, Chyawanprash, and Jeevantyadi Rasayana — recognising that macular edema is typically a long-term condition requiring ongoing supportive care. Strict dietary discipline addressing the specific systemic background — strict diabetic dietary discipline for DME (essential), low-salt diet relevant to fluid management and hypertension, antioxidant-rich Pitta-pacifying diet, avoidance of foods aggravating the systemic background. Lifestyle restoration including smoking cessation (critical for retinal vascular health), regular gentle exercise as cleared by physician, UV protection through quality sunglasses, stress management, and adequate sleep. Continued anti-VEGF schedule and ophthalmological follow-up is absolutely essential — the patient continues with their ophthalmologist for ongoing OCT monitoring, anti-VEGF management decisions, and any other ophthalmological care. Home maintenance regimen with prescribed Rasayana medicines, dietary protocols, and lifestyle measures designed to consolidate retreat gains over the months that follow — recognising that long-term outcomes in chronic macular edema develop over years of sustained care alongside continued ophthalmological management.
The 5 Core Therapies for Macular Edema Explained
1. Virechana and Systemic Pitta-Kapha-Ama Clearance Virechana is the central systemic clearing therapy for macular edema and represents the most important systemic intervention for the metabolic-inflammatory background driving the condition. For diabetic macular edema specifically — where the systemic Madhumeha-Pitta-Rakta-Ama-Kapha imbalance drives the macular pathology — Virechana addresses the foundational doshic level that anti-VEGF therapy alone cannot reach. Performed with classical herbal purgatives carefully selected for the individual doshic profile, the procedure clears systemic Pitta from the gut, liver, and circulation; reduces the chronic inflammatory mediator load contributing to retinal vascular dysfunction and increased permeability; clears the Ama burden that compounds metabolic-inflammatory pathology; supports glycaemic regulation in diabetic patients; and meaningfully reduces the systemic background that perpetuates macular edema. Dosing is calibrated carefully — particularly in diabetic patients where glycaemic state must remain stable, in patients on multiple medications, and in patients with significant comorbidities. Following Virechana, the body is in an optimised state for the subsequent specific eye-supportive therapy to act with greater effectiveness.
2. Triphala, Saptamrita Lauha, and Eye-Supportive Internal Herbal Therapy The systemic eye-protective and antioxidant pharmacology forms the foundational pharmacological backbone of integrative Ayurvedic Macular Edema care, with several herbs and formulations playing distinct roles. Triphala (Amalaki, Bibhitaki, Haritaki) provides broad antioxidant action relevant to retinal oxidative damage — Amalaki being one of the highest natural concentrations of vitamin C and providing substantial antioxidant capacity that aligns conceptually with the antioxidant rationale of modern AREDS2 supplementation in retinal disease. Saptamrita Lauha is the classical eye-protective formulation combining Triphala with Yashtimadhu and processed iron preparation, with traditional indications across multiple retinal and visual conditions. Amalaki Rasayana provides sustained antioxidant and broader Rasayana benefit. Punarnava is the most clinically important single herb for the fluid-accumulation dimension of macular edema specifically — its classical action on Sotha (oedema and pathological fluid accumulation) combined with its anti-inflammatory and tissue-protective properties provides supportive pharmacology directly relevant to the macular fluid component, complementing the anti-VEGF mechanism that targets the vascular permeability driver. Guduchi provides immunomodulatory and anti-inflammatory action particularly relevant to inflammatory dimensions of macular edema. Haridra (turmeric) and Manjistha provide additional anti-inflammatory and Rakta-purifying dimensions. Yashtimadhu provides broader Pitta-pacifying action. Classical formulations integrating these herbs — Triphala Ghrita and Mahatriphala Ghrita as eye-Rasayana ghrita preparations, Drakshadi Kashayam, Patoladi Kashayam, and others — are prescribed individually based on the specific clinical pattern, doshic profile, and underlying cause of the macular edema.
3. Netra Tarpana (Classical Eye-Supportive Therapy) Netra Tarpana is the signature Ayurvedic eye therapy, involving retention of warm medicated ghee over the eye within a contained ring constructed around the orbit with a paste of black gram flour. The patient lies supine while the warm medicated ghee bathes the eye for 15 to 30 minutes per session, with the patient slowly opening and closing the eye to allow the ghee to contact the entire ocular surface. The procedure provides gentle, sustained therapeutic action on the ocular surface tissues (cornea, conjunctiva), supports the lacrimal and meibomian gland function, and through systemic absorption effects on broader ocular tissue health. For macular edema patients, Netra Tarpana is performed only when clinically appropriate: with ophthalmologist clearance confirming the procedure is safe in the current state; when the macular edema is stable rather than in acute flare; typically at least 2 weeks after the most recent anti-VEGF injection to avoid any interaction with the post-injection state; and with appropriate aseptic technique. Ghrita selection is doshic-specific: Triphala Ghrita as the foundational eye-protective preparation; Mahatriphala Ghrita for stronger Rasayana effect; Jeevantyadi Ghrita for Pitta-dominant inflammatory presentations; Patoladi Ghrita for combined Pitta-Kapha presentations. It bears clear and honest statement: Netra Tarpana supports overall ocular tissue health and provides systemic ocular Rasayana effect through its various mechanisms — but it is not direct treatment for the macular edema fluid itself. The macular fluid is the target of anti-VEGF therapy, which addresses the vascular permeability driver. Netra Tarpana's role is supportive ocular care alongside the essential ophthalmological treatment, helping maintain overall eye health and ocular tissue integrity during the long-term course that chronic macular edema typically involves.
4. Nasya and Head-Eye Ecosystem Support Nasya — the administration of medicated oils through the nasal passage — provides supportive therapy for the broader head-eye ecosystem on which ocular function depends. Anu Taila Nasya in courses of 7 to 14 days during the retreat clears the broader head channels, supports the Vata-Pitta balance of the head region, and provides general supportive effect on the structures functionally connected to the eye through shared vascular and neural anatomy. The procedure is gentle and well-tolerated, and combines well with the other components of the macular edema treatment program.
5. Madhumeha-Specific Care and Rasayana for Long-Term Eye Support For the majority of macular edema patients — those with diabetic macular edema — addressing the underlying Madhumeha (diabetes) is foundational, not peripheral, to effective integrative care. The fifth therapeutic dimension integrates Madhumeha-specific Ayurvedic herbs alongside the eye-specific therapy: Methi (fenugreek) for glycaemic support and insulin sensitivity; Karela (bitter gourd) with its insulin-mimetic action; Vijaysar (Pterocarpus marsupium) — the premier classical anti-diabetic herb with substantial traditional and modern evidence; Gudmar (Gymnema sylvestre) with its blood-sugar-modulating action; Jamun (Syzygium cumini) seed; and classical formulations like Madhumehantaka Churna, Chandraprabha Vati, and Madhumehari Yog. These work alongside the patient's diabetes medications (which continue uninterrupted), supporting better glycaemic control which is itself one of the most important determinants of DME outcomes. Beyond the Madhumeha-specific dimension, sustained Rasayana therapy for long-term eye support continues: Chyawanprash as the premier classical Rasayana with broad systemic and antioxidant benefit; Brahma Rasayana for cognitive-systemic Rasayana effect; Jeevantyadi Rasayana for eye-specific long-term support; Triphala and Saptamrita Lauha at maintenance doses continuing the antioxidant ocular protection over the years of ongoing care that chronic macular edema typically requires. This long-term Rasayana dimension is what makes integrative care meaningful in chronic conditions where the retreat itself is only the starting point of a longer therapeutic relationship.
How Long Should an Ayurvedic Treatment Program for Macular Edema Last?
|
Therapeutic Benefit | ||
| 7–14 days | Initial systemic Pitta calming, metabolic improvement, established Punarnava-led therapy | ||
| 14–21 days | Moderate Pitta-Kapha clearance via Virechana, completed Netra Tarpana course (where clinically appropriate) | ||
| 21–28 days | Complete treatment protocol — recommended for diabetic and chronic recurrent patients | ||
| 28+ days | Long-standing DME with multi-system involvement, complex multi-factor presentations |
The exact duration of your Macular Edema treatment is decided after consultation with the Ayurvedic doctor, based on the specific cause of macular edema (DME, RVO-related, uveitic, post-surgical, wet AMD-related), current OCT findings and anti-VEGF treatment schedule, underlying systemic conditions particularly diabetes status and control, blood pressure and other vascular risk factors, overall constitutional state, and individual treatment goals. As a general guide, 14 to 28 days supports meaningful integrative care for most chronic macular edema presentations, with longer programs of 28 days or more recommended for long-standing DME with multi-system involvement, refractory recurrent macular edema, and complex multi-factor presentations. The ophthalmologist coordination is essential throughout — anti-VEGF injection schedules continue uninterrupted and the retreat timing is planned around them. Because chronic macular edema is fundamentally a long-term condition requiring ongoing care, the home regimen of prescribed Rasayana medicines, dietary discipline (particularly diabetic management for DME), continued anti-VEGF treatment, and lifestyle measures after the retreat is what genuinely supports long-term outcomes over the months and years that follow.
Book Consultation
Benefits of an Ayurvedic Treatment Retreat for Macular Edema
| Physical Benefits | Eye and Systemic Benefits | Long-Term Impact |
| Improved diabetes management and glycaemic control | Reduced systemic inflammatory burden affecting retina | Supported retinal health between anti-VEGF injections |
| Reduced metabolic toxin (Ama) load | Nourished ocular tissues through eye-Rasayana | Sustained antioxidant Rasayana support over years |
| Better blood pressure stability | Improved tear film and general eye comfort | Reduced systemic background driving DME |
| Improved overall energy and vitality | Supported Alochaka Pitta balance | Better long-term ocular tissue health |
Why Kerala is the Best Place for Macular Edema Treatment
An Ayurvedic Macular Edema treatment retreat in Kerala, India offers the most clinically authentic environment for the integrative supportive care chronic macular edema requires.
- Experienced Salakya Tantra (the classical Ayurvedic ophthalmology specialty) physicians with specific expertise in Drishti Vikara and the integrative management of chronic retinal conditions
- BAMS and MD Ayurveda-certified doctors trained in classical Netra Tarpana with appropriate aseptic technique, Nasya, and the specialised eye-Rasayana protocols macular care depends upon
- In-house preparation of classical eye-supportive formulations — Triphala Ghrita, Mahatriphala Ghrita, Jeevantyadi Ghrita, Patoladi Ghrita, Saptamrita Lauha, Amalaki Rasayana, Drakshadi Kashayam, Punarnavadi Kashayam — using authentic methods and fresh herbs
- Integrated capacity for diabetes management alongside eye care, with experienced physicians familiar with Madhumeha-specific herbs and the foundational role of glycaemic control in DME outcomes
- A long-established Kerala tradition of Salakya Tantra (Ayurvedic eye specialty) with particular depth in chronic retinal condition management
- Clear understanding that anti-VEGF therapy is non-negotiable for active macular edema and willingness to coordinate openly with the patient's ophthalmologist on injection scheduling and overall management
- Capacity for the long-term care relationships that chronic macular edema typically requires, with structured home regimens and follow-up protocols
Sri Lanka offers a comparable tropical healing environment with growing Ayurvedic expertise in chronic retinal and metabolic conditions, while Bali provides wellness-oriented treatment retreats integrating Ayurvedic eye care with holistic diabetes management and lifestyle correction. For specialised Salakya Tantra expertise and authentic classical eye-Rasayana preparations, Kerala remains the destination of choice.
Macular Edema Treatment Retreats by Location and Recommended Centres
Kerala, India — The most clinically authentic destination for Ayurvedic Macular Edema treatment, with experienced Salakya Tantra physicians and the rich Kerala tradition of classical eye care including Netra Tarpana, Nasya, and eye-Rasayana therapy. Alleppey • Kovalam • Kumarakom • Wayanad • Palakkad
Sri Lanka — Coastal Ayurveda treatment retreats offering systemic clearing through Virechana and eye-supportive therapies in a serene environment, with integrated diabetes management for DME patients. Wadduwa • Weligama • Sigiriya • Kosgoda • Bentota
Bali, Indonesia — Wellness treatment retreats integrating Ayurvedic eye care with holistic lifestyle correction, diabetes management, and stress management in scenic tropical surroundings. Ubud • Nusa Dua • Candidasa • Lovina
WellnessLoka connects you with verified centres across these destinations — with particular care to match patients with centres that have genuine Salakya Tantra expertise, integrated diabetes management capability (essential for DME patients), and clear understanding that anti-VEGF therapy continues uninterrupted alongside the integrative care.
Who Should Consider an Ayurvedic Macular Edema Treatment Retreat
Diabetic Macular Edema (DME) patients seeking to address the systemic root — Patients with established DME who recognise that addressing the underlying Madhumeha-driven systemic background — through improved glycaemic control, reduced inflammatory burden, and constitutional rebuilding — complements the essential anti-VEGF treatment by addressing what the injections cannot reach.
Patients undergoing long-term anti-VEGF therapy seeking integrative support — Those on monthly or bi-monthly anti-VEGF injections for chronic macular edema, seeking integrative care to support overall eye health, reduce systemic inflammatory background, and build long-term constitutional resilience alongside continued injection therapy.
Chronic recurrent macular edema patients — Those experiencing frequent recurrence of macular edema requiring repeated anti-VEGF cycles, seeking to address the deeper systemic background that perpetuates the recurrence pattern.
Patients with incomplete response to anti-VEGF alone — Those with persistent residual macular thickness on OCT despite optimised anti-VEGF schedules, seeking complementary care addressing the inflammatory and metabolic dimensions that anti-VEGF alone cannot reach.
Patients with multi-eye-condition presentations — Those with combined diabetic retinopathy + DME + cataract or other combined retinal conditions, benefiting from comprehensive integrative care addressing the broader eye picture.
Post-surgical macular edema patients in recovery phase — Patients recovering from Irvine-Gass syndrome or other post-surgical macular edema, where the acute treatment has been completed and integrative care supports recovery and reduces recurrence risk.
Uveitic macular edema patients between flares — Those with chronic uveitis-associated macular edema seeking integrative care during stable periods, addressing the broader inflammatory background through systemic Pitta-pacifying therapy.
Patients with significant metabolic-vascular burden — Those with combined diabetes, hypertension, dyslipidaemia, and other metabolic syndrome features driving retinal pathology, benefiting from comprehensive systemic integrative care.
Patients seeking long-term eye-Rasayana-based supportive care — Those drawn to the depth of classical Salakya Tantra care, wanting to anchor long-term eye health with sustained Triphala-Saptamrita Lauha-Amalaki-based Rasayana supervised by experienced physicians.
Patients seeking to optimise their anti-VEGF response — Those wishing to maximise the benefit of their anti-VEGF treatment by addressing the systemic background that contributes to disease activity, in coordination with their ophthalmologist.
Who Should Approach Treatment with Caution
Ayurvedic care for Macular Edema is genuinely valuable as integrative supportive care, but the absolute clinical priority is ensuring that essential ophthalmological treatment continues uninterrupted and that the boundaries of Ayurvedic care are clearly understood. A thorough consultation is essential, and Ayurvedic retreat-based care should be deferred or replaced by urgent ophthalmological treatment in cases involving:
Acute active macular edema with significant vision loss requiring immediate anti-VEGF treatment — This requires immediate ophthalmological care, not retreat-based care. Delaying indicated anti-VEGF treatment can result in irreversible vision loss as chronic edema produces permanent photoreceptor damage.
Patients without recent ophthalmological evaluation including OCT — Any macular edema patient considering integrative care must have current ophthalmological assessment with OCT to establish baseline and treatment plan.
Patients overdue for scheduled anti-VEGF injections — The scheduled injection takes absolute priority over any retreat scheduling.
Suspected new wet AMD conversion or new macular edema — New macular edema or suspected progression requires immediate ophthalmological evaluation, not retreat-based care.
Active wet AMD requiring urgent anti-VEGF initiation — This is time-critical and retreat-based care has no role until anti-VEGF treatment is established.
Recent intraocular surgery — Patients require minimum 4-6 weeks postoperative recovery before any Ayurvedic eye therapies can be considered, with explicit ophthalmologist clearance.
Patients with concurrent eye infections or other acute ocular pathology — Active ocular infection or other acute ocular conditions require resolution before integrative eye care.
Active uveitis flare — Active uveitis with macular edema requires immediate ophthalmological management; integrative care is for stable periods.
Pregnancy with significant macular edema — Pregnant patients with significant macular edema require obstetric and ophthalmological co-management; certain Ayurvedic therapies and herbs are deferred in pregnancy.
Patients with unstable diabetes — DME patients with very poorly controlled diabetes (HbA1c above 10%, frequent hypoglycaemic episodes) need diabetes stabilisation before retreat-based care.
Patients with significant cardiovascular instability — Many DME patients have significant cardiovascular comorbidity; instability requires medical management before integrative care.
Patients on complex medication regimens — Multiple medications including diabetes management, anti-hypertensives, lipid-lowering agents, anti-VEGF, and others require careful coordination of any Ayurvedic herbs through the supervising physicians.
Patients with unrealistic expectations — Those expecting Ayurveda to "dissolve" the macular edema or replace anti-VEGF treatment may benefit from clear pre-treatment counselling about realistic outcomes of integrative supportive care.
Choosing the Right Treatment Retreat for Macular Edema
Qualified Salakya Tantra (Ayurvedic ophthalmology) trained physicians — BAMS or MD Ayurveda-credentialed doctors with demonstrated experience in chronic retinal conditions and the integrative care these conditions require, not generalists applying standard wellness protocols.
Integrated diabetes management capability — Essential for DME patients (the majority of macular edema patients), with physicians experienced in Madhumeha management and capable of supporting glycaemic optimisation alongside the eye-specific care.
Clear understanding that anti-VEGF is non-negotiable — Centres whose physicians clearly understand that active macular edema requiring anti-VEGF cannot be substituted by Ayurveda, with treatment planned around continued injection schedules.
Proper facilities for safe Netra Tarpana and related eye procedures — Including appropriate aseptic technique, trained therapists, and clinical environment for the technically demanding eye procedures.
Personalised cause-specific protocols — Treatment plans matched to the specific cause of macular edema (DME, RVO-related, uveitic, post-surgical, wet AMD-related), current treatment status, OCT findings, and constitutional profile.
Authentic in-house eye-Rasayana preparations — Classical formulations including Triphala Ghrita, Mahatriphala Ghrita, Jeevantyadi Ghrita, Patoladi Ghrita, Saptamrita Lauha, Amalaki Rasayana, and Punarnava-based formulations prepared on-site using traditional methods.
Willingness to coordinate with the ophthalmologist — Centres whose physicians actively communicate with the treating ophthalmologist on anti-VEGF scheduling, treatment response, and overall management.
Capacity for long-term care relationships — Recognising that chronic macular edema requires ongoing care, with structured home regimens and follow-up protocols beyond the retreat itself.
Clear continuity-of-care planning — Centres providing detailed written guidance on continued Rasayana therapy, dietary management (particularly diabetic management), continued anti-VEGF scheduling, monitoring requirements, and lifestyle measures for the post-retreat period.
How WellnessLoka Helps You Choose the Right Ayurveda Treatment Retreat for Macular Edema
Choosing the right treatment retreat for Macular Edema benefits from clear, honest guidance about Ayurveda's supportive (not substitutive) role in this condition. WellnessLoka exists to ensure that patients can make this decision with full information, genuine guidance, and complete confidence.
Access to Verified Retreat Centres Every centre listed on WellnessLoka for Macular Edema treatment has been independently assessed for physician credentials, Salakya Tantra expertise, integrated diabetes management capability (essential for DME patients), facilities for safe Netra Tarpana and related eye procedures, and clear understanding that anti-VEGF therapy continues uninterrupted alongside integrative care. We list only centres where the integrative role of Ayurvedic care is clearly understood — where treatment supports and complements continued ophthalmological care rather than substituting for it.
Free Pre-Retreat Consultation with Our Ayurvedic Doctor Before you choose a retreat, WellnessLoka offers a complimentary consultation with our in-house Ayurvedic consultant. This consultation reviews your specific cause of macular edema (DME, RVO-related, uveitic, post-surgical, wet AMD-related), current OCT findings and anti-VEGF treatment schedule, underlying systemic conditions particularly diabetes status, blood pressure, lipid status, current medications, ophthalmologist coordination details, and overall constitutional profile. A critical part of this consultation is explicit verification that you are on an appropriate anti-VEGF schedule for active macular edema and that retreat timing accommodates your injection schedule rather than disrupting it. Based on the assessment, we match you with the retreat centre and program duration best suited for your specific cause and clinical context. It is purely a guidance consultation to help you make an informed, medically sound decision before you travel.
Transparent Centre Comparison WellnessLoka provides clear, honest information about each listed centre — physician qualifications including Salakya Tantra expertise, integrated diabetes management capability, therapy protocols, program structure, monitoring capabilities, accommodation, and pricing — allowing you to compare options across Kerala, Sri Lanka, and Bali with full clarity and confidence.
Best Price Guarantee Through our strong, long-standing relationships with partner centres, you benefit from exclusive partner pricing that is always lower than booking directly. You receive the most authentic care for your Macular Edema treatment program without paying more for it.
Retreats for Every Budget From luxury wellness resorts to affordable, authentic healing centres, WellnessLoka helps you find a Macular Edema treatment retreat that aligns perfectly with your comfort level and budget — without ever compromising on the specialised Salakya Tantra expertise this condition benefits from.
Treatment is in Expert Hands Once you arrive at your chosen retreat, your Macular Edema treatment program is fully designed and managed by the qualified Ayurvedic physicians at that centre. From your first in-person consultation onwards, all clinical decisions, daily monitoring, therapeutic adaptation, and medical management are guided by experienced doctors on the ground — physicians with deep training in Salakya Tantra and direct, hands-on familiarity with the specialised classical eye therapies your program involves, alongside integrated capacity for the diabetes management that DME patients require. Your treatment unfolds under continuous, qualified supervision.
Local Support Team Our on-ground experts assist you at every step, from your first enquiry through to the completion of your retreat — resolving any issues that arise and ensuring your entire Macular Edema healing journey runs smoothly and safely.
End-to-End Booking Support From your first enquiry to confirmed booking, WellnessLoka provides full administrative and logistical support — ensuring a smooth, stress-free process so that you can focus entirely on preparing for your healing program.
Why Travellers Trust WellnessLoka WellnessLoka is rated 4.9? on Google, with verified reviews from wellness travellers who have experienced authentic Ayurveda healing through us. We are trusted by hundreds of travellers from 28+ countries across Europe, the Americas, Asia, Australia, and Africa, backed by over a decade of expertise in curating authentic Ayurveda retreats across trusted centres. Our dedicated support team is available 24×7 to assist you before, during, and after your Macular Edema treatment retreat.
Begin Your Healing Journey
Macular Edema sits in that important clinical space where modern ophthalmology has produced genuinely transformative treatment — anti-VEGF therapy has, within two decades, converted what was a leading cause of irreversible vision loss into a treatable condition with often-preserved central vision — and yet where the underlying systemic dimensions remain substantially beyond what the retinal-level interventions alone can reach. The patient with diabetic macular edema continues on monthly injections in part because the systemic metabolic-inflammatory background driving the macular pathology continues; the patient with RVO-related edema receives anti-VEGF for the macula while the underlying vascular dysfunction continues; the patient with chronic recurrent macular edema cycles through repeated treatment courses without addressing the deeper background. The anti-VEGF treatment is absolutely cornerstone, vision-saving, and must never be substituted by anything else — and within this clear framing, a meaningful role exists for integrative supportive care addressing what the injections cannot reach.
Gentle, restorative Ayurvedic care offers what may be a meaningful contribution to this deeper picture: addressing the systemic Madhumeha-Pitta-Rakta-Kapha-Ama background that drives diabetic macular edema through Virechana and integrated diabetes management; supporting overall ocular tissue through classical Triphala-Saptamrita Lauha-Amalaki antioxidant Rasayana that aligns with the antioxidant logic of modern retinal care; integrating Punarnava-based therapy specifically for the fluid-pathology dimension that complements the anti-VEGF mechanism; providing gentle classical eye-supportive therapy through Netra Tarpana when clinically appropriate; rebuilding constitutional Ojas through sustained Rasayana — always alongside the continued anti-VEGF treatment and ophthalmological care that remain the foundation of management. Whether you choose a treatment retreat in Kerala, Sri Lanka, or Bali, Ayurvedic care for Macular Edema offers a thoughtful, deeply integrative path to supported eye health, addressed systemic background, and constitutional resilience — always undertaken as a complement to, and never a replacement for, the essential ophthalmological care that protects your vision.


