
When Hunger Pain Strikes: An Ayurvedic Path to Duodenal Healing and Lasting Relief
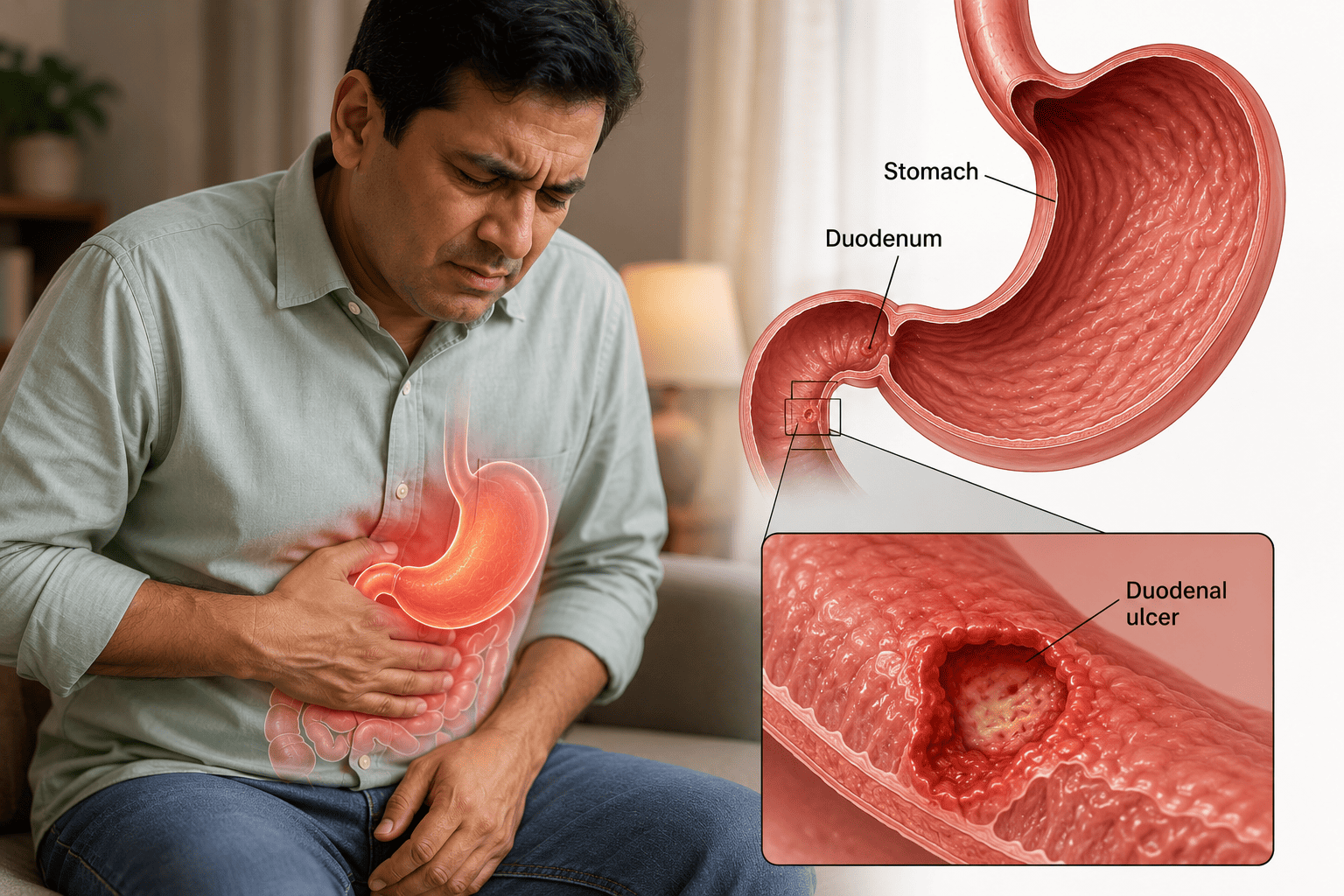
Duodenal Ulcer represents the most common type of peptic ulcer disease, accounting for approximately 70-80% of all peptic ulcers, with substantial impact on quality of life and broader wellbeing. The condition involves open sores in the lining of the duodenum (first part of the small intestine just past the stomach), exposing underlying tissue to gastric acid producing the characteristic pain patterns and various complications. Duodenal ulcers occur predominantly in adults aged 30-50, are more common in men, and have distinctive clinical features that distinguish them from gastric ulcers — most notably the classic pattern of pain relieved by eating and pain worsening 2-3 hours after meals or at night (often awakening patients), reflecting the relationship to gastric acid production cycles.
The clinical presentation classically involves epigastric burning pain with characteristic timing — pain typically begins 2-3 hours after eating when gastric acid production peaks and food has largely emptied from stomach, with pain relief upon eating (food and antacid effects) being a distinguishing feature from gastric ulcers. Nocturnal pain awakening patients from sleep is common and characteristic. Associated symptoms include hunger pangs, bloating, belching, nausea (less common than gastric ulcers), and various complications when severe. Complications can be serious including bleeding (most common complication, manifesting as melena/black stools or hematemesis), perforation (life-threatening surgical emergency, particularly in anterior wall ulcers), gastric outlet obstruction from chronic scarring (less common with modern treatment), and rarely penetration into adjacent organs.
Primary causes are similar to gastric ulcers but with some distinctions: H. pylori infection (most common cause, present in 70-95% of duodenal ulcers), NSAID use (substantial cause), stress (both psychological and physiological), smoking (substantial risk factor for both development and impaired healing), excessive acid production (sometimes constitutional), genetic predisposition (stronger family history association than gastric ulcers), and rarely specific conditions like Zollinger-Ellison syndrome. Duodenal ulcers reflect predominantly acid hypersecretion combined with mucosal vulnerability, while gastric ulcers more often reflect normal/reduced acid with mucosal compromise.
Modern management is similar to gastric ulcers including diagnostic evaluation (upper endoscopy with H. pylori testing — biopsy less critical than gastric ulcers since duodenal malignancy is rare), H. pylori eradication therapy when present (cornerstone treatment), acid-suppressing medications (PPIs as primary treatment with substantial effectiveness for duodenal ulcers), NSAID modification, lifestyle modifications, and monitoring. Duodenal ulcers generally heal more readily than gastric ulcers and recurrence prevention through H. pylori eradication and lifestyle modifications is highly effective.
While conventional treatment is effective for most patients, substantial therapeutic gaps and complementary roles exist where Ayurveda offers genuine value:
Patients with chronic recurrent duodenal ulcers — Despite H. pylori eradication, some patients experience recurrent episodes benefiting from comprehensive integrative approach.
Patients with persistent symptoms despite PPI therapy — Continued discomfort seeking comprehensive approach.
Patients seeking to reduce long-term PPI dependence — Comprehensive approach potentially enabling reduced medication needs.
Patients with stress-related duodenal ulcer patterns — Substantial stress contributing significantly.
Patients with Pitta-predominant constitutional patterns — Pitta predominance often particularly relevant given duodenal ulcer's strong acid-related pathology.
Patients with NSAID-induced duodenal ulcers — Comprehensive integrative approach for those requiring continued NSAIDs.
Patients with PPI side effects — Those experiencing PPI-related issues seeking alternatives.
Patients seeking comprehensive digestive wellness — Holistic approach to long-term digestive health.
Patients post-H. pylori eradication — Recovery support and recurrence prevention.
Patients with associated conditions — GERD, gastritis, functional dyspepsia often co-occurring.
Classical Ayurveda addresses duodenal ulcers within the framework of Parinama Shoola (cyclical/transformation-related pain), Annadrava Shoola (food-related pain), and broader Amlapitta (acidic Pitta) framework, with substantial Pitta-predominant pathology and Pachaka Pitta (digestive Pitta) vitiation. The classical Parinama Shoola description with its characteristic cyclical pattern remarkably matches duodenal ulcer presentation. The therapeutic approach includes Yashtimadhu (Licorice) as foundational ulcer-healing herb; Shatavari for cooling Pitta-pacifying mucosal support; Avipattikara Churna as classical anti-acidic formulation; comprehensive Pitta-pacifying constitutional approach; specific anti-inflammatory and mucosal-protective approach; comprehensive lifestyle integration including stress management; coordination with continued gastroenterology care essential.
A Duodenal Ulcer treatment retreat is best understood as comprehensive integrative care undertaken for patients with confirmed duodenal ulcer disease seeking constitutional optimization, recovery support, and prevention of recurrence, alongside continued gastroenterology care including any H. pylori eradication and appropriate medication management.
What is Duodenal Ulcer?
Duodenal Ulcer is an open sore or break in the protective mucosal lining of the duodenum (first part of the small intestine), exposing underlying tissue to gastric acid and digestive enzymes.
Definition and characteristics:
- Open sore in duodenum (typically first portion/duodenal bulb)
- Most common type of peptic ulcer (70-80% of peptic ulcers)
- More common in men, ages 30-50
- Classic pain pattern: relieved by eating, worsens 2-3 hours after meals or at night
- Substantial association with H. pylori infection
- Generally heals more readily than gastric ulcers
- Recurrence common without H. pylori eradication
Classification:
By location within duodenum:
- Duodenal bulb ulcer — Most common location (>90%)
- Post-bulbar ulcer — Less common, may suggest specific conditions like Zollinger-Ellison syndrome
By severity and complications:
- Uncomplicated — Pain without acute complications
- Bleeding — Most common complication
- Perforation — Life-threatening emergency (particularly anterior wall ulcers)
- Penetration — Into pancreas or other organs
- Gastric outlet obstruction — From chronic scarring (less common now)
By underlying cause:
- H. pylori-associated — Most common (70-95% globally)
- NSAID-induced — Substantial cause
- Stress-related
- Idiopathic — Without identifiable specific cause
- Other causes — Rarely, Zollinger-Ellison syndrome, others
Pathophysiology:
- Imbalance between aggressive factors (gastric acid, pepsin, H. pylori, NSAIDs) and protective factors (duodenal mucus, bicarbonate, mucosal blood flow, prostaglandins)
- Acid hypersecretion often more prominent than in gastric ulcers
- H. pylori producing chronic duodenitis and mucosal damage
- Gastric metaplasia in duodenum allowing H. pylori colonization
- NSAIDs inhibiting protective prostaglandins
- Genetic and constitutional predisposition
Common symptoms:
- Epigastric burning pain with characteristic patterns
- Pain relieved by eating (food and antacid effects)
- Pain worsening 2-3 hours after meals
- Nocturnal pain (often awakening patient from sleep) — highly characteristic
- Hunger pangs
- Bloating
- Belching
- Nausea (less common than gastric ulcers)
- Sometimes asymptomatic until complications
Warning signs requiring urgent attention:
- Vomiting blood or coffee-ground material
- Black tarry stools (melena) — common with duodenal ulcer bleeding
- Severe persistent abdominal pain
- Signs of perforation (sudden severe pain, rigid abdomen)
- Significant weight loss
- Persistent symptoms despite treatment
Risk factors:
- H. pylori infection (strongest factor)
- NSAID use
- Smoking (substantial risk factor)
- Family history (stronger than for gastric ulcers)
- Younger to middle-aged adults
- Male gender
- Excessive alcohol
- Chronic stress
- Severe physiological stress
- Specific medical conditions
- Excessive caffeine
- Type O blood (modest association)
Diagnosis:
- Detailed history — Pain pattern often diagnostic
- Physical examination
- Upper endoscopy (EGD) — Definitive diagnosis
- H. pylori testing — Essential including urea breath test, stool antigen, biopsy testing
- Imaging — Sometimes upper GI series in selected cases
- Laboratory tests — Complete blood count, others as indicated
- Biopsy — Less critical for duodenal ulcers (malignancy rare in duodenum) than gastric ulcers
Modern medical management:
- H. pylori eradication when present (cornerstone)
- Acid-suppressing medications (PPIs primary)
- NSAID modification when contributing
- Lifestyle modifications
- Treatment of complications
- Generally good response to treatment
Understanding Parinama Shoola and Amlapitta: The Ayurvedic Root of Duodenal Ulcer
The Ayurvedic understanding of duodenal ulcer sits within the framework of Parinama Shoola (cyclical/transformation-related abdominal pain), Annadrava Shoola (food-related pain), and broader Amlapitta (acidic Pitta), with substantial Pitta-predominant pathology and Pachaka Pitta (digestive Pitta) vitiation. The classical description of Parinama Shoola with its characteristic cyclical pattern remarkably matches modern duodenal ulcer presentation.
Core concepts:
Parinama Shoola — Classical Description Matching Duodenal Ulcer:
The classical description of Parinama Shoola provides remarkably accurate correspondence to duodenal ulcer presentation:
- Cyclical pattern corresponding to ulcer pain cycles
- Pain timing related to digestion phases corresponding to duodenal ulcer's characteristic timing
- Pain at specific intervals after meals matching duodenal ulcer's 2-3 hour post-meal pattern
- Variation with food consumption matching the relief-with-eating pattern
- Substantial classical literature addressing this specific pattern
Pachaka Pitta as Central — Pachaka Pitta governing digestion located in stomach and upper small intestine — exactly the anatomical region of duodenal ulcers. Vitiation produces the inflammatory acidic ulcerative pattern.
Amlapitta Framework — Classical concept of "acidic Pitta" with substantial classical literature addressing hyperacidity and ulcer-spectrum conditions:
- Urdhwaga Amlapitta — Upward-moving (with GERD patterns sometimes accompanying)
- Adhoga Amlapitta — Downward-moving (often corresponding to duodenal patterns)
- Substantial therapeutic content in classical texts
Annadrava Shoola — Food-related pain patterns with classical recognition of food's variable effects on abdominal pain.
Sub-types based on doshic predominance:
- Pitta-predominant — Most common; burning quality, heat patterns, particularly relevant for duodenal ulcer
- Pitta-Vata — Combined with anxiety, stress dimensions, common in stressed patients
- Tridoshic — Complex mixed patterns
Agni Considerations:
- Tikshnagni (sharp/excessive digestive fire) producing burning patterns — particularly relevant for duodenal ulcer with acid hypersecretion
- Vishamagni (irregular digestion) in stress-related patterns
Manasika Bhava Dimensions:
- Substantial recognition of stress, anger (Krodha), grief (Shoka), anxiety affecting Pachaka Pitta
- Anticipating modern understanding of stress-ulcer relationships
- Particularly important given duodenal ulcer's stress associations
Predisposing Nidana classical Ayurveda identifies:
- Excessive spicy, sour, salty foods
- Excessive hot, sharp foods
- Irregular eating patterns (particularly missing meals — relevant given duodenal ulcer's relationship to empty stomach)
- Eating before previous meal digested
- Chronic stress, anger, grief
- Excessive alcohol (Madya)
- Smoking and tobacco (substantial Pitta aggravation)
- Excessive caffeine
- Constitutional Pitta predominance
- Sleep irregularities including late-night eating then sleeping
- Excessive heat exposure
This comprehensive understanding shapes the Ayurvedic approach: address Pitta-predominant pathology through comprehensive Pitta pacification; support Pachaka Pitta restoration through specific digestive-supportive herbs; promote mucosal healing through cooling demulcent herbs (Yashtimadhu particularly important); manage acid hypersecretion through specific approaches; address Manasika Bhava dimensions through comprehensive stress management; support regular meal patterns essential for duodenal ulcer management; coordinate with continued gastroenterology care for proper diagnosis confirmation, H. pylori treatment when needed, and broader medical management.
The 3 Stages of Ayurvedic Treatment for Duodenal Ulcer
1. Preparation (Purva Karma) Comprehensive assessment including duodenal ulcer history (endoscopic confirmation, H. pylori status, recurrence pattern, complications), current symptoms with attention to characteristic timing patterns, current medications (PPIs, antibiotics for H. pylori), NSAID use history, smoking status, alcohol use, stress patterns, dietary patterns including meal timing, and constitutional profile. Gastroenterology coordination essential — sharing treatment approach, ensuring continued appropriate medications, coordinating H. pylori treatment, planning follow-up as needed.
Diagnostic confirmation essential — Endoscopic confirmation with H. pylori testing.
Initial constitutional support with foundational Pitta-pacifying approach.
Initial dietary modifications — Beginning Pitta-pacifying patterns, eliminating ulcer-aggravating foods, regular meal timing absolutely essential for duodenal ulcer management.
Foundational lifestyle measures — Stress management initiation, smoking cessation absolutely essential, alcohol elimination, NSAID modification where possible.
2. Core Treatment (Pradhana Karma) Primary therapies focus on five coordinated lines:
Comprehensive Pitta-Pacifying Constitutional Approach with Specific Meal Pattern Emphasis:
- Cool, mild, easily digestible dietary patterns
- Reduced spicy, sour, salty foods (substantially acid-aggravating)
- Reduced caffeine
- Regular meal timing absolutely essential — irregular eating particularly problematic for duodenal ulcer
- Smaller frequent meals often beneficial for duodenal ulcer — keeping food in stomach buffering acid
- Bedtime snack consideration — sometimes valuable given nocturnal pain pattern (light easily digestible foods)
- Adequate cooling foods
- Specific Pitta-pacifying herbs and spices (fennel, coriander, cardamom, cumin)
- Avoiding very hot foods
Comprehensive Herbal Therapy with Ulcer-Healing Emphasis:
Foundational ulcer-healing herbs:
- Yashtimadhu (Glycyrrhiza glabra/Licorice) — Foundational with substantial classical use and modern clinical evidence for ulcer healing, mucosal protection, anti-inflammatory effects, and H. pylori-supportive effects; particularly valuable for duodenal ulcers
- Shatavari — Cooling demulcent mucosal protection
- Amalaki — Gentle support with vitamin C
- Guduchi — Immune and broader support
- Bilwa — Specific digestive support
- Musta — Digestive support
Classical formulations:
- Avipattikara Churna — Classical anti-acidic preparation particularly valuable
- Yashtimadhu preparations
- Shatavari Ghrita — Ghee preparation with cooling effects
- Sukumara Ghrita — Comprehensive support
- Praval Pishti — Coral preparation for acidity
- Mukta Pishti — Pearl preparation in selected applications
- Kamadhenu Rasa
- Specific combinations matched to individual presentation
Demulcent and Mucosal Protective Approach:
- Yashtimadhu preparations providing direct mucosal protection
- Shatavari for cooling demulcent effects
- Milk-based preparations in moderation
- Ghee in moderation for cooling and protective effects
- Specific cooling beverages
Comprehensive Stress Management:
- Recognition of substantial stress contributions particularly for duodenal ulcer
- Meditation with documented benefits
- Yoga adapted to needs
- Pranayama (Sheetali particularly valuable, Bhramari for relaxation)
- Avoidance of intense pranayama during active ulcer
- Structured stress reduction
- Specific Manasika Bhava herbs (Brahmi, Jatamansi, Shankhpushpi)
- Particular attention to anger (Krodha) management given Pitta-anger associations
Comprehensive Lifestyle Integration with Critical Smoking Emphasis:
- Smoking cessation absolutely essential — substantial impact on duodenal ulcer healing and recurrence; particularly important for duodenal ulcer
- Alcohol elimination essential
- NSAID avoidance or modification with prescribing physicians
- Regular meal timing with smaller frequent meals
- Adequate sleep — particularly important for duodenal ulcer given nocturnal symptoms
- Stress management as central element
- Regular gentle exercise (avoiding intense exercise during active ulcer)
- Caffeine moderation or elimination
- Avoidance of late-night heavy eating but consideration of light bedtime snack given nocturnal pain pattern
Coordination with Continued Gastroenterology Care:
- Continued prescribed PPIs throughout treatment
- H. pylori eradication treatment essential when present — must be completed
- Follow-up testing for H. pylori eradication (typically 4-8 weeks after antibiotic completion)
- Potential PPI reduction with gastroenterology guidance as integrative care produces benefits
- Recognition that duodenal ulcers generally heal more readily than gastric ulcers with appropriate treatment
3. Rejuvenation (Paschat Karma) Sustained constitutional support, continued lifestyle modifications particularly smoking cessation and meal timing, continued ulcer-healing herbal therapy, continued stress management, periodic clinical follow-up, continued gastroenterology coordination, and recognition that recurrence prevention through comprehensive approach is highly valuable particularly for chronic recurrent ulcer patterns.
The 5 Core Therapies for Duodenal Ulcer Explained
1. Yashtimadhu-Led Comprehensive Ulcer-Healing Herbal Therapy Yashtimadhu (Glycyrrhiza glabra/Licorice) represents one of the most clinically valuable single Ayurvedic herbs for duodenal ulcer with substantial classical use and rigorous modern clinical evidence supporting ulcer-healing effects. Modern clinical evidence demonstrates substantial benefits including direct ulcer healing through mucosal protection, increased mucus production, prostaglandin enhancement, anti-inflammatory effects, antibacterial effects against H. pylori, and broader gastric protective effects — particularly valuable for duodenal ulcers given their predominantly acid-related pathology. DGL (Deglycyrrhizinated Licorice) preparations particularly valuable for sustained use. Combined with comprehensive ulcer-healing herbal approach: Shatavari providing cooling demulcent effects; Amalaki for vitamin C and antioxidant effects; Guduchi for immune and broader support; Bilwa for specific digestive support; Musta for digestive function. Classical formulations: Avipattikara Churna as foundational classical anti-acidic preparation particularly valuable for duodenal ulcers given acid hypersecretion role; standard administration 3-5g twice daily before meals; Shatavari Ghrita for sustained cooling demulcent effects; Yashtimadhu Churna combinations; Sukumara Ghrita for comprehensive support; Praval Pishti and Mukta Pishti in appropriate clinical situations for substantial acidity reduction. Standard administration: Yashtimadhu 1-3g daily of authentic preparations or DGL 760mg before meals; continued 2-3 months minimum for ulcer healing with sustained benefits over longer periods for recurrence prevention. Quality considerations essential. WellnessLoka centres provide authentic in-house preparation.
2. Comprehensive Pitta-Pacifying Constitutional Approach with Critical Meal Pattern Integration Comprehensive Pitta-pacifying constitutional approach with specific attention to meal patterns is particularly important for duodenal ulcer given its strong relationship to gastric acid production cycles and food timing. Dietary Pitta pacification with duodenal ulcer-specific considerations: Regular meal timing absolutely essential — irregular eating particularly problematic given duodenal ulcer's relationship to empty stomach and acid production cycles; Smaller frequent meals often particularly beneficial for duodenal ulcer — keeping food in stomach buffering acid and preventing the empty-stomach acid attack pattern; Light bedtime snack consideration — sometimes valuable given duodenal ulcer's nocturnal pain pattern, with easily digestible foods (warm milk, banana, oats) buffering nocturnal acid; Cool, mild, easily digestible foods as foundation; Reduced spicy, sour, salty foods essential; Reduced caffeine with substantial impact on acid production; Adequate cooling foods: coconut water, cucumber, milk in moderation, ghee in moderation; Specific Pitta-pacifying herbs and spices: fennel, coriander, cardamom, cumin, curry leaves. Specific foods often beneficial: Banana, almonds, milk, oats (excellent for duodenal ulcer), coconut water, bottle gourd, white rice; Foods to specifically avoid: Excessive citrus, tomatoes, vinegar, chocolate, peppermint, fried foods, very spicy foods, alcohol, excessive caffeine. Lifestyle Pitta pacification: Avoiding overheating, cool environment, adequate hydration, appropriate clothing. Constitutional considerations: For Pitta-predominant individuals — sustained lifelong Pitta pacification essential.
3. Comprehensive Stress Management Addressing Substantial Stress-Ulcer Dimensions Comprehensive stress management is particularly important for duodenal ulcer given substantial stress-ulcer relationships with stress affecting acid secretion, mucosal blood flow, and immune function. Substantial recognition of stress-ulcer relationships in duodenal ulcer: Both psychological stress and physiological stress substantially affecting duodenal ulcer development, recurrence, and symptom severity; particular relevance for Type-A personalities and high-stress occupational patterns; bidirectional relationships between stress and symptoms. Comprehensive stress management approach: Meditation with documented benefits — MBSR, transcendental meditation, others; Yoga adapted to ulcer management: Gentle restorative practices preferred; Avoidance during active ulcer: intense practices, deep abdominal compression poses, intense backbends; Pranayama practices: Sheetali (cooling breath) particularly valuable for Pitta-related conditions; Bhramari for relaxation; Anulom Vilom for balance; Avoidance of intense pranayama (Kapalabhati, Bhastrika) during active ulcer; Structured stress reduction practices. Specific Manasika Bhava herbs: Brahmi for cognitive and emotional support; Jatamansi for anxiety; Shankhpushpi for mental-emotional balance; Saraswatarishtam for nervous system support; Ashwagandha used cautiously initially. Addressing specific psychological dimensions: Anger (Krodha) management — particularly important given Pitta-anger associations; Perfectionism patterns common in Type-A duodenal ulcer patients; Work-life balance addressing chronic occupational stress; Recognition that professional mental health support beneficial for substantial stress dimensions.
4. Comprehensive Lifestyle Integration with Absolute Smoking Cessation Emphasis Comprehensive lifestyle integration with particular emphasis on smoking cessation is essential for duodenal ulcer management given smoking's substantial impact on duodenal ulcer development, healing, and recurrence. Smoking cessation absolutely essential: Smoking substantially impairs duodenal ulcer healing (smokers heal 50% slower than non-smokers), increases recurrence dramatically (recurrence rates substantially higher in smokers), produces broader digestive harm, and impairs H. pylori treatment effectiveness; comprehensive cessation support including behavioral approaches, nicotine replacement consideration where appropriate, addressing underlying stress and other contributors to smoking; Recognition that without smoking cessation, ulcer management substantially compromised. Alcohol elimination essential: Substantial irritant effects; impaired healing; worsened H. pylori effects; complete elimination during active treatment and substantial moderation thereafter. NSAID management critical: Coordination with prescribing physicians; alternative pain management where possible (acetaminophen alternatives for many indications); when NSAIDs must continue, comprehensive gastric protection essential. Regular meal timing absolutely essential for duodenal ulcer given relationship to empty stomach acid attack: smaller frequent meals; avoidance of long gaps; consideration of bedtime snack for nocturnal symptoms. Adequate sleep with attention to nocturnal pain: Often disturbed in duodenal ulcer patients; addressing sleep disruption from pain; sometimes elevated head positioning beneficial; bedtime snack consideration. Regular gentle exercise: Beneficial for stress and broader health; avoid intense exercise during active ulcer. Caffeine moderation or elimination: Substantial impact on acid production. Environmental and occupational considerations: Addressing chronic work stress where contributing.
5. Coordination with Continued Gastroenterology Care and H. pylori Eradication Focus Coordination with continued gastroenterology care is essential for comprehensive duodenal ulcer management with particular emphasis on H. pylori eradication given its central role in duodenal ulcer pathogenesis. Diagnostic confirmation essential: Endoscopic confirmation; H. pylori testing through appropriate methods; biopsy less critical for duodenal ulcers than gastric ulcers (malignancy rare in duodenum); evaluation for atypical features suggesting Zollinger-Ellison or other conditions in selected cases. H. pylori eradication when present — cornerstone treatment: Triple or quadruple antibiotic regimens as standard care — substantially effective for duodenal ulcer with high cure rates; must be completed regardless of integrative care; integrative supportive role during antibiotic treatment including probiotic-like fermented foods, immune support, antioxidant approaches; post-eradication confirmation with retest typically 4-8 weeks after treatment completion — essential to verify cure given recurrence risk if treatment failed; recognition that successful H. pylori eradication substantially reduces recurrence risk making this absolutely central to duodenal ulcer management. PPI management: Continued throughout active treatment; duodenal ulcers generally respond well to PPI therapy with healing rates >95% with appropriate treatment; potential reduction with gastroenterology guidance after H. pylori eradication confirmed and healing achieved; never abrupt discontinuation. Recurrence prevention focus: Recognition that successful H. pylori eradication plus comprehensive lifestyle modifications (particularly smoking cessation) substantially reduces recurrence; sustained constitutional approach addressing underlying patterns particularly valuable for the small proportion of patients with continued recurrence despite H. pylori eradication. Recognition of complications requiring urgent care: Bleeding (melena common with duodenal ulcers, hematemesis), perforation (sudden severe pain — particularly anterior wall duodenal ulcers), obstruction — all requiring urgent gastroenterology evaluation. Long-term framework: Recognition that comprehensive duodenal ulcer management with H. pylori eradication and lifestyle modifications generally produces excellent long-term outcomes; integrative approach providing supportive role for sustained digestive wellness.
How Long Should an Ayurvedic Treatment Program for Duodenal Ulcer Last?
| Duration | Therapeutic Benefit | |||
|
Initial protocols established, ulcer-healing therapy initiation, foundational lifestyle integration | |||
| 14–21 days | Comprehensive constitutional support, established protocols, substantial symptom improvement | |||
| 21–28 days | Extended program for substantial constitutional rebuilding and comprehensive integration | |||
| 2–3 months home regimen | Sustained therapy for complete ulcer healing |
The exact duration is decided after consultation with the Ayurvedic doctor in coordination with continued gastroenterology care, based on H. pylori status, recurrence history, comorbidities, current medications, treatment goals, and individual factors. Initial intensive retreat 14-28 days establishing protocols. Continued home regimen 2-3 months minimum for complete ulcer healing with sustained constitutional support for recurrence prevention. Follow-up endoscopy typically not routinely required for uncomplicated duodenal ulcers (unlike gastric ulcers) but H. pylori eradication confirmation essential. Recognition that duodenal ulcers with H. pylori eradication and lifestyle modifications generally have excellent prognosis — integrative approach valuable for sustained wellness and recurrence prevention.
Benefits of an Ayurvedic Treatment Retreat for Duodenal Ulcer
| Physical Benefits | Functional and Digestive Benefits | Long-Term Impact | ||
| Reduced ulcer pain and symptoms | Improved digestion and appetite | Substantially reduced recurrence risk | ||
| Improved ulcer healing | Better quality of sleep (reduced nocturnal pain) | Foundation for sustained digestive wellness | ||
| Reduced stress and anxiety |
|
Better long-term gastrointestinal health | ||
| Better overall vitality |
|
|
Why Kerala is the Best Place for Duodenal Ulcer Treatment
An Ayurvedic Duodenal Ulcer treatment retreat in Kerala, India offers the most clinically authentic environment for comprehensive Parinama Shoola and Amlapitta care.
- Experienced physicians with specific expertise in classical digestive disorders and Pitta-related conditions
- BAMS and MD Ayurveda-certified doctors with gastrointestinal Ayurveda training
- Specialised practitioner training in Pitta-pacifying therapies
- In-house preparation of classical formulations — Avipattikara Churna, Yashtimadhu preparations, Shatavari Ghrita, Sukumara Ghrita, Praval Pishti, Mukta Pishti, and various ulcer-supportive preparations — using authentic methods and fresh herbs
- Authentic in-house preparation of supportive oils and preparations
- Proper facilities for comprehensive integrative care with appropriate medical supervision
- Capacity for integrated care including coordination with continued gastroenterology
- Long-established Kerala tradition of comprehensive digestive Ayurveda
- Capacity for sustained long-term care relationships
- Coordination capability with continued gastroenterology and broader specialist care
- Integrated meal preparation following Pitta-pacifying protocols with regular meal timing
- Capacity for psychological dimensions integration given substantial stress components
Sri Lanka offers complementary tropical healing environment, while Bali provides wellness-oriented treatment retreats. For specialised digestive Ayurveda with comprehensive Pitta-pacifying expertise, Kerala offers the deepest tradition.
Duodenal Ulcer Treatment Retreats by Location and Recommended Centres
Kerala, India — The most clinically authentic destination for classical digestive Ayurvedic care with established Pitta-pacifying tradition. Alleppey • Kovalam • Kumarakom • Wayanad • Palakkad
Sri Lanka — Coastal Ayurveda treatment retreats with comprehensive supportive care. Wadduwa • Weligama • Sigiriya • Kosgoda • Bentota
Bali, Indonesia — Wellness treatment retreats integrating Ayurvedic care with holistic wellness. Ubud • Nusa Dua • Candidasa • Lovina
WellnessLoka connects you with verified centres offering genuine digestive Ayurveda expertise, authentic Pitta-pacifying preparations, comprehensive integrative care capability, willingness to coordinate with continued gastroenterology care, and clear understanding of integrative role.
Who Should Consider an Ayurvedic Duodenal Ulcer Treatment Retreat
Patients with confirmed duodenal ulcer disease — Seeking comprehensive constitutional approach to support healing and prevention.
Patients with chronic recurrent duodenal ulcers — Despite H. pylori eradication, recurring episodes benefit from comprehensive integrative approach.
Patients post-H. pylori eradication — Recovery support and recurrence prevention.
Patients with NSAID-induced duodenal ulcers — Those requiring continued NSAID use seeking gastric protection.
Patients with stress-related duodenal ulcer patterns — Substantial stress contributing significantly.
Patients with persistent symptoms despite PPI therapy — Continued discomfort seeking comprehensive approach.
Patients with PPI side effects — Those experiencing PPI-related issues.
Patients seeking to reduce long-term PPI dependence — Comprehensive approach potentially enabling reduced needs.
Patients with Pitta-predominant constitutional patterns — Substantial constitutional dimensions.
Patients with associated conditions — GERD, gastritis, functional dyspepsia co-occurring.
Patients with substantial nocturnal symptoms — Comprehensive approach addressing characteristic patterns.
Patients seeking comprehensive digestive wellness — Long-term holistic approach.
Patients in recovery from complications — Post-bleeding recovery with continued specialist care.
Patients with anxiety and ulcer dimensions — Combined approach for both.
Patients seeking integrative philosophy — Classical Ayurvedic depth informing health approach.
Who Should Approach Treatment with Caution
Ayurvedic care for Duodenal Ulcer is genuinely valuable for most patients, but appropriate medical evaluation and continued gastroenterology coordination are essential:
Patients with suspected active GI bleeding — Melena, hematemesis require urgent medical attention, not retreat-based care.
Patients with suspected perforation — Sudden severe abdominal pain requires emergency care.
Patients without proper diagnostic confirmation — Should have endoscopic confirmation before retreat-based care.
Patients with active H. pylori infection without treatment — Should complete eradication therapy alongside integrative care; should not delay or substitute antibiotic treatment.
Patients with severe acute symptoms — May need stabilization before retreat.
Patients with significant comorbidities — Require careful coordination.
Patients on anticoagulation or with bleeding risk — Require careful coordination given complication risks.
Patients planning to discontinue PPIs abruptly — Should taper with gastroenterology guidance.
Patients requiring continued NSAIDs without alternatives — May need continued conventional gastric protection.
Patients with severe psychiatric illness — Require appropriate mental health care.
Patients with active substance use disorders — Require addiction treatment alongside integrative care.
Patients with suspected Zollinger-Ellison syndrome — Recurrent multiple ulcers, post-bulbar location, severe symptoms may suggest this rare condition requiring specialized evaluation.
Patients unwilling to address smoking — Continued smoking substantially limits outcomes for duodenal ulcer management.
Patients with unrealistic expectations — Honest counseling about continued importance of conventional treatment particularly H. pylori eradication.
Patients considering self-prescription — Expert consultation essential.
Patients without continued gastroenterology care — Integrative care complements rather than replaces specialist management.
Choosing the Right Treatment Retreat for Duodenal Ulcer
Qualified physicians with digestive Ayurveda expertise — BAMS or MD Ayurveda-credentialed doctors with specific training in Pitta-related conditions and digestive disorders.
Specialised practitioners trained in Pitta-pacifying therapies — Including appropriate techniques.
Authentic in-house herbal preparations — Including specific ulcer-supportive formulations particularly Avipattikara Churna, Yashtimadhu preparations, Shatavari Ghrita, and classical preparations.
Proper infrastructure — Including appropriate facilities for digestive care.
Capacity for integrated dietary support with regular meal timing — Essential given the critical importance of meal patterns for duodenal ulcer; structured meal preparation following Pitta-pacifying protocols with appropriate timing.
Coordination capability with continued gastroenterology care — Essential for H. pylori management and ongoing care.
Capacity for psychological dimensions integration — Essential given substantial stress components.
Capacity for sustained long-term care relationships — Recognising recurrence prevention focus.
Honest framing — Centres clearly understanding integrative role.
Clear continuity-of-care planning — Detailed home regimens, follow-up timing, dietary guidance.
Privacy and discretion — Essential for digestive health concerns.
How WellnessLoka Helps You Choose the Right Ayurveda Treatment Retreat for Duodenal Ulcer
Choosing the right treatment retreat for Duodenal Ulcer benefits from specialised guidance. WellnessLoka exists to ensure that patients can make this decision with full information, genuine guidance, and complete confidence.
Access to Verified Retreat Centres Every centre listed on WellnessLoka for Duodenal Ulcer treatment has been independently assessed for physician credentials, specialised digestive Ayurveda expertise, authentic preparation of Pitta-pacifying and ulcer-supportive formulations, comprehensive integrative care infrastructure, structured meal timing capability, willingness to coordinate with continued gastroenterology care, and clear understanding of the integrative role. We list only centres practising authentic care with appropriate honesty about realistic expectations.
Free Pre-Retreat Consultation with Our Ayurvedic Doctor Before you choose a retreat, WellnessLoka offers a complimentary consultation with our in-house Ayurvedic consultant. This consultation reviews your specific context (ulcer history with endoscopic confirmation, H. pylori status, current medications, recurrence patterns, lifestyle factors particularly smoking and stress, treatment goals) and matches you with the appropriate centre. Honest framing about realistic expectations and continued gastroenterology care importance.
Transparent Centre Comparison Clear, honest information about each listed centre — physician qualifications, digestive expertise, therapy protocols, program structure, dietary protocols, and pricing.
Best Price Guarantee Through our strong partner relationships, exclusive partner pricing always lower than booking directly.
Retreats for Every Budget From luxury wellness resorts to authentic healing centres without compromising on specialised expertise.
Treatment is in Expert Hands Your program is fully managed by qualified Ayurvedic physicians with specialised digestive training and direct familiarity with ulcer management approaches.
Local Support Team Our on-ground experts assist you at every step ensuring smooth treatment journey.
End-to-End Booking Support From enquiry to confirmed booking, full administrative and logistical support.
Why Travellers Trust WellnessLoka WellnessLoka is rated 4.9? on Google, with verified reviews. Trusted by hundreds of travellers from 28+ countries, backed by over a decade of expertise. Dedicated support team available 24×7.
Begin Your Healing Journey
Duodenal Ulcer represents the most common type of peptic ulcer disease with characteristic clinical features and predominantly acid-related pathology, with substantial impact on quality of life despite the advances in modern medical management. The modern medical landscape has substantially advanced through clear identification of H. pylori as primary cause, highly effective eradication therapy, effective acid-suppressing medications particularly PPIs which produce healing rates >95% in duodenal ulcers, and improved diagnostic tools. The combination of H. pylori eradication and lifestyle modifications particularly smoking cessation generally produces excellent long-term outcomes. Yet despite these substantial advances, real therapeutic gaps remain: patients with chronic recurrent ulcers despite H. pylori eradication, patients with persistent symptoms despite appropriate treatment, patients seeking to reduce long-term PPI dependence with associated effects, patients with substantial stress-related dimensions, and patients seeking holistic philosophy informing broader digestive wellness.
Within this clinical context, classical Ayurvedic care offers meaningful integrative contributions through the Parinama Shoola and Amlapitta framework — the classical Parinama Shoola description with its characteristic cyclical pain pattern remarkably matches duodenal ulcer presentation, reflecting sophisticated classical clinical observation. The therapeutic framework includes Yashtimadhu-led comprehensive ulcer-healing herbal therapy combining substantial classical use with rigorous modern clinical evidence; comprehensive Pitta-pacifying constitutional approach with critical attention to meal patterns essential for duodenal ulcer management; comprehensive stress management addressing the substantial stress-ulcer dimensions; comprehensive lifestyle integration with particular emphasis on smoking cessation (substantial impact on duodenal ulcer outcomes), alcohol elimination, NSAID modification, and broader factors; coordination with continued gastroenterology care absolutely essential particularly for H. pylori eradication which represents cornerstone of modern duodenal ulcer management.
Whether you choose a treatment retreat in Kerala, Sri Lanka, or Bali — with Kerala offering particular depth in classical digestive Ayurveda — Ayurvedic care for Duodenal Ulcer offers a thoughtful, deeply integrative path to comprehensive digestive wellness and effective recurrence prevention. The integrative approach is undertaken in close coordination with continued conventional gastroenterology care, recognising that comprehensive duodenal ulcer management includes both classical Ayurvedic depth and modern medical expertise (particularly H. pylori eradication) where each genuinely benefits the patient. Investment in comprehensive integrative care for duodenal ulcer represents investment in broader digestive and constitutional health — addressing not just immediate ulcer healing but the underlying constitutional, lifestyle, and stress-related factors determining long-term digestive wellness.
The journey to comprehensive ulcer healing and sustained digestive wellness extends beyond just acute treatment — encompassing comprehensive attention to constitutional factors, dietary patterns including critical meal timing, smoking cessation, stress management, lifestyle factors, and the foundation for sustained digestive and broader health across the lifespan with substantially reduced recurrence risk through comprehensive approach.


